Type 1 diabetes (T1D) is not just an insulin deficiency—it is a precision disease. When glucose runs high chronically, complications accelerate. When glucose is normalized, risks plummet.
A growing number of families are rediscovering an old truth: carbohydrate restriction dramatically simplifies blood glucose control.
Across studies and real-world practice, reducing carbohydrates to <30–50g/day has been associated with:
-
HbA1c levels in the non-diabetic range (<5.7%)
-
50–70% lower insulin requirements
-
Dramatically reduced glucose variability
-
Fewer hypoglycemic crashes
-
Improved triglycerides and HDL
Let’s explore how we got here—and why this approach is resurfacing.
History Restored: Before High-Carb Guidelines
The Pre-Insulin Era

-
John Rollo (1797) removed starches and sugars from the diet, prolonging survival.
-
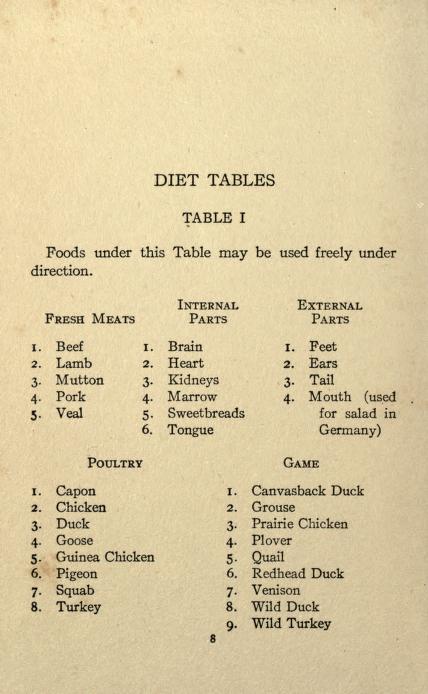
Frederick Madison Allen (1910s) used strict carbohydrate restriction to prevent ketoacidosis and extend life.
Patients lived lean, carb-restricted lives until insulin became available in 1921.
Early Insulin + Low Carb
When insulin was introduced, physicians paired it with low-carbohydrate diets. The goal was simple:
Small carbohydrate intake → small insulin dose → small margin of error.
This minimized hypoglycemia and severe hyperglycemia.
The High-Carb Shift
By the 1950s–1970s, dietary fat fears reshaped guidelines. The American Diabetes Association (ADA) eventually endorsed 45–65% of calories from carbohydrates.
Insulin doses rose.
Glucose variability widened.
Complications remained common.
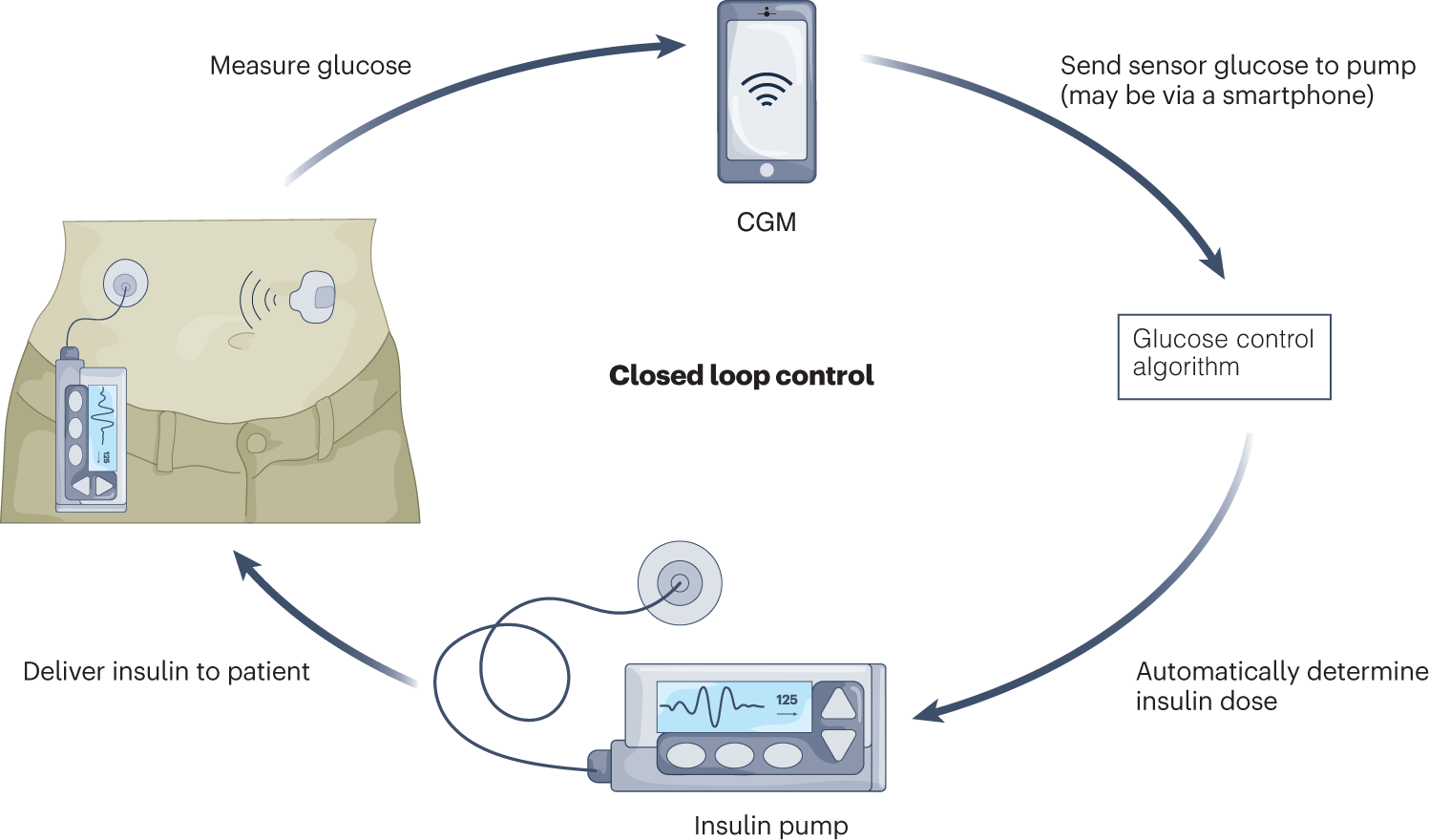
The Modern Tech Paradox
-
Continuous Glucose Monitors (CGMs)
-
Insulin pumps
-
Hybrid closed-loop systems
But average HbA1c in many large registries remains around 8% (≈183 mg/dL).
Typical improvements:
-
Pumps: −0.3% HbA1c
-
CGM: −0.2 to −0.7%
-
Closed loop: often 7–7.5% average
Helpful tools—but rarely normalization.
Technology manages glucose swings.
Carbohydrate restriction reduces the swings in the first place.
The Carb–Glucose Lock
Carbohydrates convert to glucose rapidly. Quality matters less than quantity.
-
200g carbs/day → 100–150 units insulin common
-
<30–50g carbs/day → 20–40 units typical
-
High carb → 100–120 mg/dL daily swings
-
Low carb → flatter CGM lines
Smaller inputs = smaller mistakes.
Evidence for Very-Low-Carb in T1D

-
HbA1c 5.1–5.9% on 0–50g carbohydrate
-
Insulin reductions up to 70%
-
Lower triglycerides (often −40–50%)
-
Higher HDL
-
Stable growth in children (normal height z-scores)
Safety findings across studies:
-
No increased DKA rates when insulin is appropriately maintained
-
No increased severe hypoglycemia
-
Improved triglyceride/HDL ratios
-
Nutrient sufficiency achievable with eggs, meat, fish, liver, dairy, and non-starchy vegetables
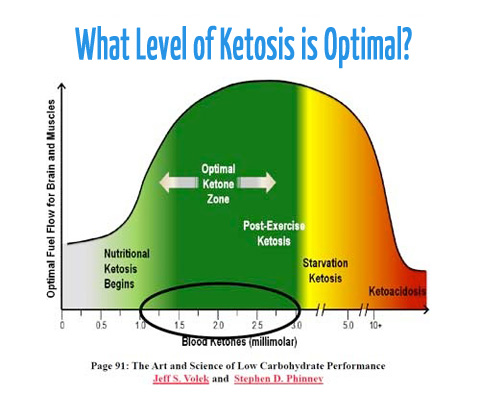
Ketones fuel up to 70% of brain energy needs.
Gluconeogenesis supplies essential glucose steadily.
Carbohydrates are not biologically essential.
A Practical Low-Carb Reboot
For carb-heavy food cultures, practical swaps matter.
Suhoor/ Breakfast
-
Eggs with Paneer cooked in ghee
-
Beef kabab cooked with butter
-
Fish + butter
(~5–8g carbs)
Iftar/ Dinner
-
Mutton seekh kebab
-
Bhindi (okra) or keema karela
-
Full Fat Yogurt
(~10–15g carbs)
Skip:
-
Roti
-
Rice
-
Naan
-
Sugary drinks
Result:
-
Fewer boluses
-
Lower insulin totals
-
Less volatility
In many families, insulin use drops 50–70%, reducing cost burden significantly.
Why This Works
The core principle mirrors the approach advocated by Richard K. Bernstein, who has lived with T1D for over nine decades:
“Small inputs make small mistakes.”
Carbohydrate restriction:
-
Reduces insulin dose size
-
Reduces absorption mismatch
-
Reduces glucose variability
-
Reduces oxidative stress
-
Lowers HbA1c into non-diabetic ranges
And normalization of glucose is strongly associated with reduced microvascular and macrovascular complications.
The Big Picture
Standard high-carb diabetes management often aims for “acceptable control.”
Low-carbohydrate strategies aim for normal physiology.
History shows it worked before insulin.
Modern CGM data shows it works now.
For families navigating T1D:
-
Technology is helpful.
-
Insulin is life-saving.
-
But diet determines the size of the challenge.
Rediscovering carbohydrate restriction is not extreme—it is historically grounded metabolic logic.
Normalize glucose.
Stabilize variability.
Reclaim lifespan.
The strategy is simple:
Start with the next meal.
References
- https://www.youtube.com/channel/UCuJ11OJynsvHMsN48LG18Ag
- https://www.youtube.com/watch?v=dPd78PnsQNA
- https://www.youtube.com/watch?v=4X7IwzFPn_Q
- https://www.youtube.com/watch?v=qQc2H26T98E&t=469s
- https://www.youtube.com/watch?v=3xdlzHyysNk&t=7s
- https://www.youtube.com/watch?v=3xdlzHyysNk&list=PLs_TA02I6IvX_FakgvWkfziEciqRSgZnz
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://www.youtube.com/watch?v=3xdlzHyysNk&t=7s
- https://www.youtube.com/watch?v=3xdlzHyysNk&list=PLs_TA02I6IvX_FakgvWkfziEciqRSgZnz
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://www.youtube.com/watch?v=3xdlzHyysNk&t=7s
- https://www.youtube.com/watch?v=3xdlzHyysNk&list=PLs_TA02I6IvX_FakgvWkfziEciqRSgZnz
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://www.youtube.com/watch?v=3xdlzHyysNk&t=7s
- https://www.youtube.com/watch?v=3xdlzHyysNk&list=PLs_TA02I6IvX_FakgvWkfziEciqRSgZnz
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://www.youtube.com/watch?v=vyOI9bk3VZc
- https://www.youtube.com/watch?v=um0Ly12Wia8
- https://www.youtube.com/watch?v=zJGAbZIvRh8
- https://www.youtube.com/watch?v=GdmK_SCA2ls
- https://www.youtube.com/watch?v=fA1qh4Sty8g
- https://www.youtube.com/watch?v=zJGAbZIvRh8
- https://www.youtube.com/watch?v=Ho9-oD9KSiw
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://www.facebook.com/Type1Grit/
- https://www.jci.org/articles/view/142246