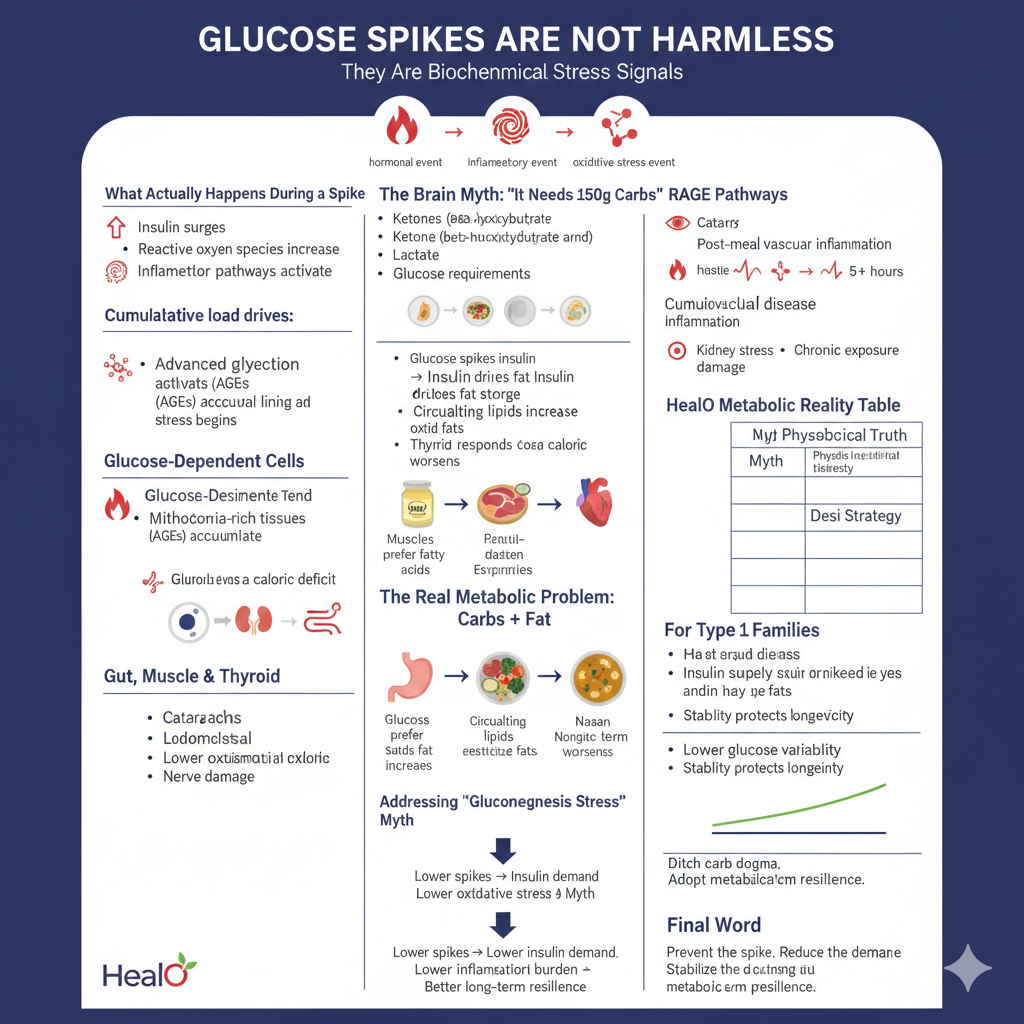
They Are Biochemical Stress Signals
A glucose spike is not “just energy.”
It is a hormonal event.
An inflammatory event.
An oxidative stress event.
Repeated daily spikes — especially in insulin-resistant or diabetes-prone individuals — accelerate metabolic damage far beyond the meal itself.
In Pakistan, where 150–300g carbohydrate intake daily is common, this matters.
What Actually Happens During a Spike
When glucose surges:
• Insulin surges
• Reactive oxygen species increase
• Inflammatory pathways activate
• Advanced glycation end products (AGEs) accumulate
• Vascular lining stress begins
RAGE (Receptor for Advanced Glycation End Products) pathways remain activated for hours — not minutes — particularly in insulin-resistant states.
In some individuals, post-meal vascular inflammation can persist 5+ hours.
Three meals.
Three spikes.
Chronic exposure.
This cumulative load drives:
• Cataracts
• Cardiovascular disease
• Kidney stress
• Nerve damage
Not instantly — but progressively.
The Brain Myth: “It Needs 150g Carbs”
The brain does not require 150g of dietary carbohydrate.
Under fat-adapted conditions:
• Ketones (beta-hydroxybutyrate) can supply ~60–70% of brain energy
• Lactate contributes efficiently
• Glucose requirement drops significantly
Even mild nutritional ketosis (~0.5 mmol/L BHB) improves mitochondrial efficiency and reduces oxidative stress compared to high-glucose flux.
This is metabolic flexibility — not starvation.
“But What About Glucose-Dependent Cells?”
Certain cells (like red blood cells) lack mitochondria and must use glucose.
However:
• The body produces ~30g glucose daily via gluconeogenesis
• Primary substrate is recycled lactate (Cori cycle)
• Not muscle breakdown under normal fed conditions
Gluconeogenesis is demand-driven — not automatic protein destruction.
Well-formulated low-carb eating does not cause muscle wasting when protein intake is adequate.
Gut, Muscle & Thyroid — Clarifying the Fear
Muscles prefer fatty acids at rest.
Mitochondria-rich tissues oxidize fats and ketones efficiently.
The thyroid responds more to caloric deficit and stress than carbohydrate absence.
The “carbs are mandatory” narrative confuses optional fuel with essential fuel.
The Real Metabolic Problem: Carbs + Fat
High carbohydrate + high fat meals create the perfect storm:
Glucose spikes insulin →
Insulin drives fat storage →
Circulating lipids increase →
Resistance worsens
Ghee alone does not spike insulin.
Meat + vegetables remains stable.
Naan + curry overloads both pathways.
HealO Metabolic Reality Table
| Myth | Physiological Truth | Desi Strategy |
|---|---|---|
| Brain needs 150g carbs | Ketones cover majority of fuel needs | Ghee + fish, meat, egg-based meals |
| Spikes are harmless if levels drop | Inflammation persists for hours | <50g carbs daily framework |
| Protein turns into stress glucose | Lactate recycling dominates | Adequate beef, mutton, eggs |
| Carbs + fat balance each other | Promotes storage, resistance | Protein-fat structured meals |
For Type 1 Families
Every spike requires insulin.
Every insulin surge influences:
• Fat storage
• Resistance development
• Variability
• Long-term vascular stress
Lower glucose variability:
• Reduces bolus size
• Shrinks error margin
• Improves predictability
• Protects vessels over decades
Stability protects longevity.
Addressing the “Gluconeogenesis Stress” Myth
Gluconeogenesis increases appropriately during fat adaptation.
It is regulated by need — not by panic.
Muscle catabolism occurs only in:
• Severe caloric deficit
• Starvation
• Advanced illness
Not in structured, protein-adequate low-carb nutrition.
HealO Principle
Metabolism heals when volatility decreases.
Lower spikes →
Lower insulin demand →
Lower oxidative stress →
Lower inflammatory burden →
Better long-term resilience
This is not extreme.
It is controlled fuel input.
Final Word
Glucose spikes are not neutral events.
They are cumulative signals.
In a population already facing high diabetes prevalence, the strategy is not “cover the spike.”
The strategy is:
Prevent the spike.
Reduce the demand.
Stabilize the system.
Ditch all dogma.
Adopt metabolic precision.
References
- https://www.frontiersin.org/journals/cardiovascular-medicine/articles/10.3389/fcvm.2020.570553/full?s=09
- https://pubmed.ncbi.nlm.nih.gov/16848698/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5315230/?s=09
- Recent Post