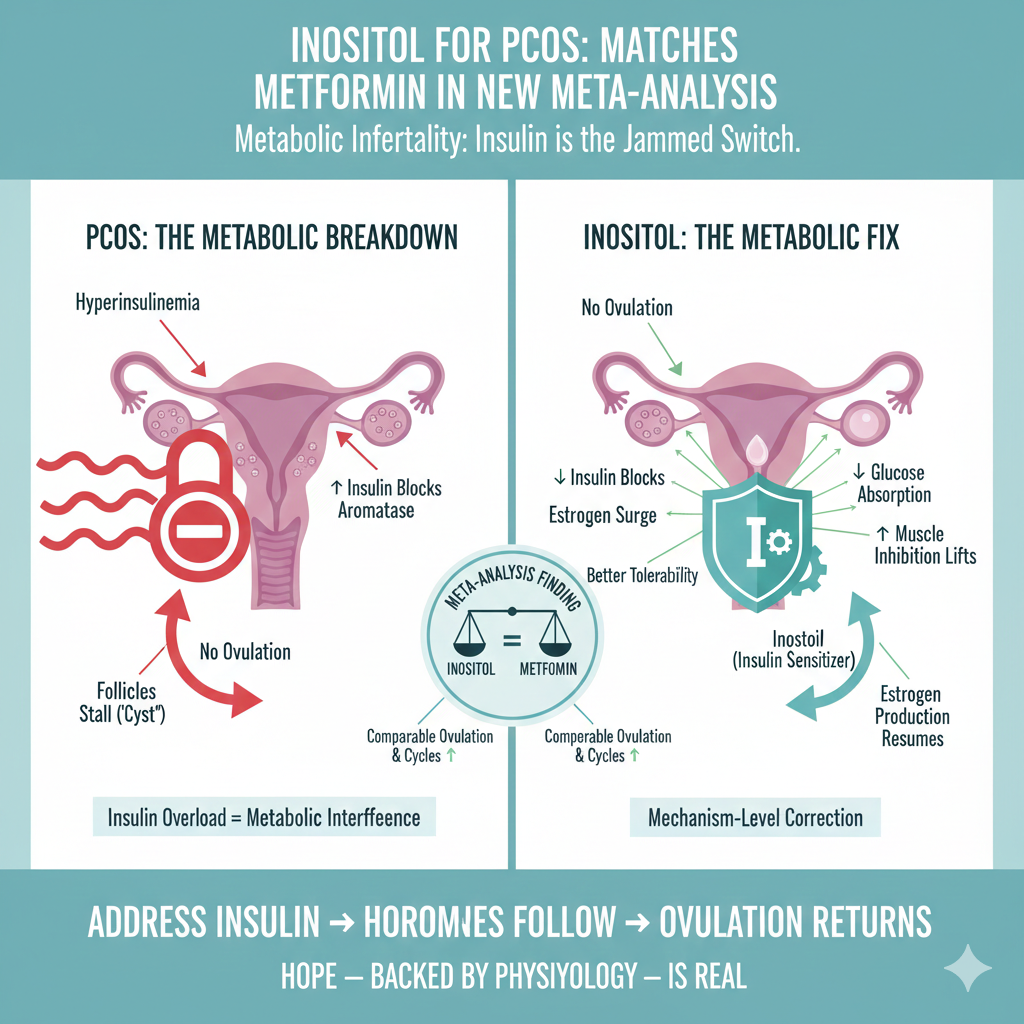
Matches Metformin in New Meta-Analysis
PCOS isn’t a “cyst problem.” It’s metabolic infertility—and insulin is the jammed switch.
PCOS: The Metabolic Breakdown (Why Ovulation Stalls)
At the core of PCOS is insulin overload. Chronically high insulin doesn’t just affect blood sugar—it blocks ovarian hormone flow.
What insulin does in PCOS
Hyperinsulinemia suppresses aromatase, the enzyme that converts testosterone → estrogen
No estrogen surge → no dominant follicle
Ovulation never fires → follicles stall and accumulate as “cysts”



Think of it like this
Normal cycle: Follicles compete → estrogen peaks → one ovulates, the rest dissolve
PCOS cycle: Insulin jams aromatase → estrogen stays low → no ovulation → follicles linger
PCOS is not ovarian failure.
It’s metabolic interference.
Inositol: An Insulin Sensitizer That Targets the Root
Inositol (myo-inositol ± D-chiro-inositol) is a vitamin-like insulin signaling molecule, not a hormone.
What it actually does
↓ intestinal glucose absorption → smaller glucose spikes
↑ muscle glucose uptake → lower circulating insulin
Improves insulin signaling inside cells
Downstream effect
Aromatase inhibition lifts
Estrogen production resumes
Ovulation probability rises
This is mechanism-level correction—not symptom masking.
The Game-Changer: Inositol vs Metformin
A recent meta-analysis comparing inositol with metformin (the long-standing PCOS gold standard) found:
Equivalent improvements in insulin resistance
Comparable ovulation and cycle restoration
Better tolerability for many women (less GI distress)
Effective dosing
2–4 g/day (often split doses)
Many OTC products are underdosed → read labels
Always coordinate dosing with your clinician
This is not “supplement fluff.”
This is pharmacologic-level metabolic therapy.
Low-Carb + Inositol: Metabolic Synergy
Inositol works best when insulin pressure is already falling.
Why low-carb amplifies results
Fewer carbs → less glucose → less insulin
Inositol then enhances insulin sensitivity further
Ovarian signaling finally clears
Foundation matters
Protein-forward meals (eggs, fish, meat)
Stable fats
Minimal refined carbs/sugars
Think of inositol as the signal repair tool—low-carb removes the signal noise.
Bottom Line
PCOS is metabolic, not mysterious
Insulin overload blocks ovulation
Inositol directly targets that block
Meta-analysis shows it performs on par with metformin
Combined with carb reduction, it can be a fertility unlock
PCOS is not a dead end.
Address insulin → hormones follow → ovulation returns.
Talk with your doctor about dosing and fit.
Hope—backed by physiology—is very real here.
2 Responses