
It is about how much glucose circulates in the bloodstream — every hour, every day, for decades.
Despite modern tools like pumps and CGMs, average HbA1c globally remains high. And that chronic elevation quietly drives long-term damage.
This is the conversation most families are not having clearly enough.
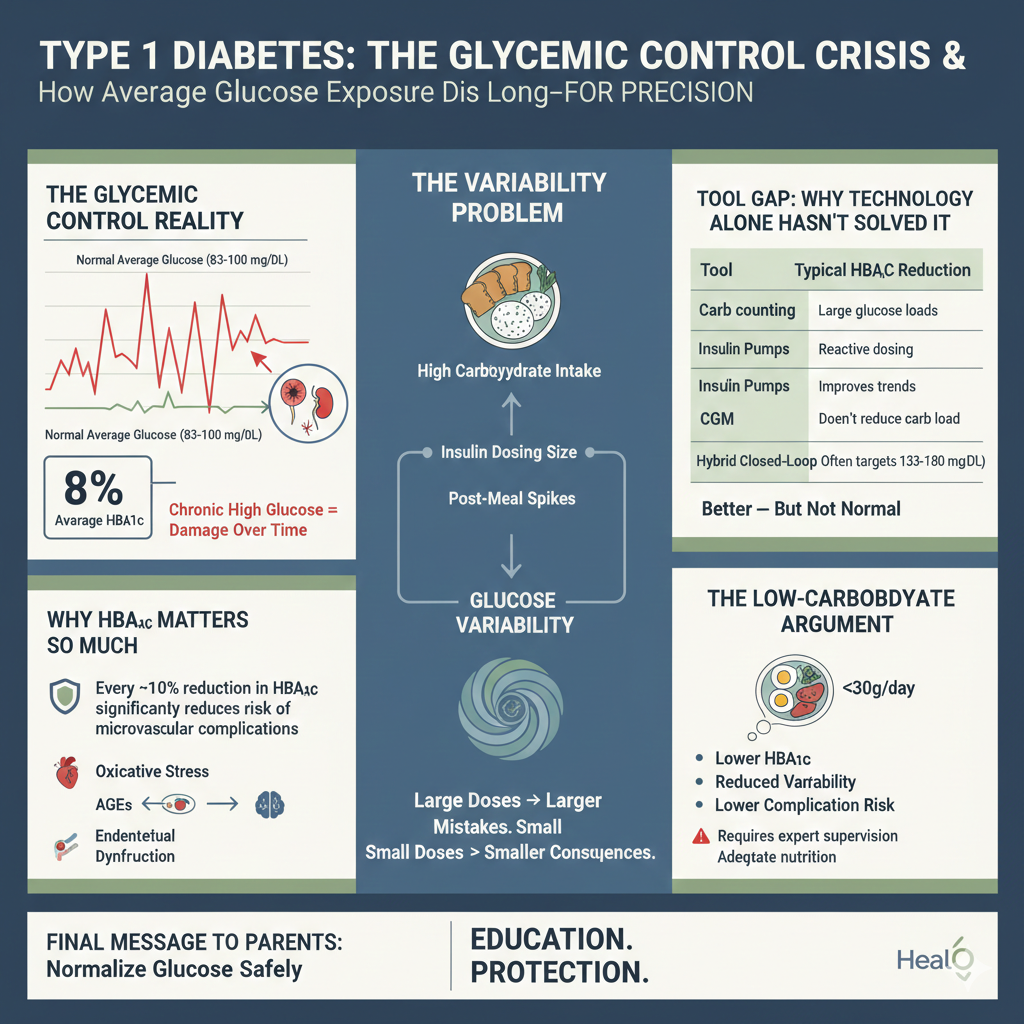
The Glycemic Control Reality
Large registry data — including cohorts from the T1D Exchange — show average HbA1c levels around 8% in many populations.
An HbA1c of 8% corresponds to an average glucose of approximately 183 mg/dL (10.2 mmol/L).
For context:
• Normal average glucose ≈ 83–100 mg/dL
• Many T1D patients live 60–100 mg/dL above physiologic levels
• Daily swings of 50–60 mg/dL are common
Globally, a significant proportion of individuals with T1D fall in the 7.5–9% HbA1c range.
Children and adolescents often have the highest averages due to growth hormones, puberty-related insulin resistance, and behavioral factors.
This is not a failure of families.
It is a structural problem in how we approach management.
Why HbA1c Matters So Much
The landmark Diabetes Control and Complications Trial and its follow-up Epidemiology of Diabetes Interventions and Complications demonstrated a powerful truth:
Every ~10% reduction in HbA1c significantly reduces risk of microvascular complications.
Lower HbA1c was associated with:
• Reduced retinopathy progression
• Reduced nephropathy
• Reduced neuropathy
Glucose exposure is dose-dependent toxicity.
Chronic hyperglycemia generates:
• Oxidative stress
• Advanced glycation end-products (AGEs)
• Endothelial dysfunction
• Microvascular damage
Over decades, this accumulates.
Mortality & Long-Term Risk
Population-based cohorts such as those led by Araz Rawshani and Shona Livingstone demonstrate sobering trends:
• All-cause mortality several-fold higher than general population
• Markedly increased cardiovascular disease risk
• Shortened life expectancy — particularly with early-onset T1D
Cardiovascular disease remains a leading cause of death.
Chronic kidney disease risk rises with persistent hyperglycemia.
Retinopathy affects a large proportion of long-standing cases.
These outcomes correlate strongly with glucose exposure over time.
The Tool Gap: Why Technology Alone Hasn’t Solved It
| Tool | Typical HbA1c Reduction | Limitation |
|---|---|---|
| Carb counting | Modest | Still large glucose loads |
| Insulin pumps | ~0.3% | Reactive dosing |
| CGM | Improves trends | Does not reduce carb load |
| Hybrid closed-loop | ~0.5–0.6% | Often targets 130–180 mg/dL |
| Islet transplant | Temporary normalization | Rejection, immunosuppression |
Technology improves safety and reduces hypoglycemia risk.
But most systems are designed around:
Managing high carbohydrate intake safely — not eliminating the glycemic load itself.
Even modern closed-loop systems often target glucose ranges well above physiologic fasting levels.
The result?
Better — but not normal.
The Variability Problem



• Insulin dosing size
• Margin of dosing error
• Post-meal spikes
• Hypoglycemia risk from overcorrection
Large doses → larger mistakes.
Smaller doses → smaller consequences.
This principle is sometimes referred to as the “law of small numbers.”
Glucose variability itself may independently contribute to oxidative stress beyond mean glucose alone.
The Low-Carbohydrate Argument
Some clinicians — notably Richard K. Bernstein — advocate very-low-carbohydrate strategies (<30g/day) to minimize glucose excursions.
Reported outcomes in adherent individuals include:
• Lower HbA1c (sometimes near non-diabetic range)
• Reduced glycemic variability
• Fewer severe hypoglycemia episodes
• Improved time-in-range
The core logic:
Less carbohydrate →
Less insulin required →
Less variability →
Lower oxidative burden →
Lower complication risk.
However, critical caveats:
• Requires low-carb physician supervision/ self training
• Must ensure adequate nutrition (especially in children)
• Growth monitoring is essential
• Psychological sustainability matters
• Individualization is non-negotiable
This is not a casual dietary shift.
It is a structured metabolic strategy.
A HealO Perspective for T1D Families
In Pakistan, access to pumps and closed-loop systems is limited by cost.
CGMs are improving access but remain expensive.
Diet, however, is modifiable.
Reducing refined carbohydrates — white rice overload, roti stacking, sugary drinks — can dramatically reduce post-meal spikes.
Even moderate carbohydrate reduction can:
• Improve time-in-range
• Lower insulin requirements
• Reduce variability
• Ease daily management burden
The goal is not perfection.
The goal is stability.
What Truly Determines Long-Term Outcome?
Not the brand of pump.
Not the insulin type alone.
Not the technology dashboard.
But:
• Average glucose exposure
• Variability
• Years spent above physiologic levels
Duration × Degree of Hyperglycemia = Complication Risk
That equation has not changed in 100 years.
Final Message to Parents
Your child’s diagnosis is not their destiny.
But chronic high glucose is not benign.
Technology helps.
Education empowers.
Precision protects.
Lowering HbA1c safely — while minimizing variability — is the most powerful lever available today.
Whether through structured carb reduction, advanced tech, or a combination:
The objective remains the same:
Normalize glucose as closely and safely as possible — for decades.
That is how lifespan is reclaimed.
References
- https://diatribe.org/understanding-diabetes/can-people-type-1-diabetes-also-get-type-2
- https://www.sciencedirect.com/science/article/pii/S016882271630153X
- https://dom-pubs.onlinelibrary.wiley.com/doi/abs/10.1111/dom.13848
- https://www.sciencedirect.com/science/article/abs/pii/S1043276006002633
- https://www.scribd.com/document/920635243/Dr-Bernsteins-Diabetes-Solution
- https://archive.org/details/isbn_9780316182690
- https://www.youtube.com/channel/UCuJ11OJynsvHMsN48LG18Ag
- https://www.youtube.com/watch?v=dPd78PnsQNA
- https://www.youtube.com/watch?v=4X7IwzFPn_Q
- https://www.youtube.com/watch?v=qQc2H26T98E&t=469s
- https://www.youtube.com/watch?v=3xdlzHyysNk&t=7s
- https://www.youtube.com/watch?v=3xdlzHyysNk&list=PLs_TA02I6IvX_FakgvWkfziEciqRSgZnz
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://www.youtube.com/watch?v=3xdlzHyysNk&t=7s
- https://www.youtube.com/watch?v=3xdlzHyysNk&list=PLs_TA02I6IvX_FakgvWkfziEciqRSgZnz
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://www.youtube.com/watch?v=3xdlzHyysNk&t=7s
- https://www.youtube.com/watch?v=3xdlzHyysNk&list=PLs_TA02I6IvX_FakgvWkfziEciqRSgZnz
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://www.youtube.com/watch?v=3xdlzHyysNk&t=7s
- https://www.youtube.com/watch?v=3xdlzHyysNk&list=PLs_TA02I6IvX_FakgvWkfziEciqRSgZnz
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://www.youtube.com/watch?v=vyOI9bk3VZc
- https://www.youtube.com/watch?v=um0Ly12Wia8
- https://www.youtube.com/watch?v=zJGAbZIvRh8
- https://www.youtube.com/watch?v=GdmK_SCA2ls
- https://www.youtube.com/watch?v=fA1qh4Sty8g
- https://www.youtube.com/watch?v=zJGAbZIvRh8
- https://www.youtube.com/watch?v=Ho9-oD9KSiw
- https://www.youtube.com/watch?v=3PZno7Nkuuw
- https://professional.diabetes.org/diapro/glucose_calc
- https://t1dexchange.org/pages/
- http://care.diabetesjournals.org/content/39/12/e214
- https://jamanetwork.com/journals/jamaophthalmology/article-abstract/635006?redirect=true
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3867999/
- https://www.ncbi.nlm.nih.gov/pubmed/9850487
- http://care.diabetesjournals.org/content/34/8/1843
- https://jamanetwork.com/journals/jama/fullarticle/2656808
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31506-X/fulltext
- https://www.mayoclinic.org/diseases-conditions/hyperglycemia/symptoms-causes/syc-20373631
- https://www.mayoclinic.org/diseases-conditions/hypoglycemia/symptoms-causes/syc-20373685
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31506-X/fulltext
- https://www.ncbi.nlm.nih.gov/pubmed/29532512
- https://jamanetwork.com/journals/jama/fullarticle/2088852
- http://care.diabetesjournals.org/content/early/2016/05/14/dc15-2399
- https://www.nejm.org/doi/full/10.1056/NEJMoa1408214
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31506-X/fulltext
- https://jamanetwork.com/journals/jama/fullarticle/2088852
- https://www.ncbi.nlm.nih.gov/pubmed/29532512
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3462745/
- https://www.ncbi.nlm.nih.gov/pubmed/16567818
- https://jamanetwork.com/journals/jama/fullarticle/2088852
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4826427/
- https://jamanetwork.com/journals/jama/fullarticle/2088852
- https://www.ncbi.nlm.nih.gov/pubmed/29532512
- https://www.ncbi.nlm.nih.gov/pubmed/29532512
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217477/
- https://www.ncbi.nlm.nih.gov/pubmed/11956379
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)31506-X/fulltext
- https://www.ncbi.nlm.nih.gov/pubmed/27925333
- https://jamanetwork.com/journals/jama/fullarticle/2088852
- https://www.ncbi.nlm.nih.gov/pubmed/29532512
- https://www.alzheimersanddementia.com/article/S1552-5260(15)02297-9/abstract
- https://jamanetwork.com/journals/jama/fullarticle/2088852
- https://www.ncbi.nlm.nih.gov/pubmed/29532512
- https://www.ncbi.nlm.nih.gov/pubmed/25767718
- https://jamanetwork.com/journals/jama/fullarticle/2088852
- https://www.ncbi.nlm.nih.gov/pubmed/29532512
- https://jamanetwork.com/journals/jama/fullarticle/2088852
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4138899/
- http://care.diabetesjournals.org/content/early/2015/07/01/dc15-0041
- https://www.sciencedirect.com/science/article/pii/S1056872718301090
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5111534/
- https://www.ncbi.nlm.nih.gov/pubmed/29573221
- https://www.ncbi.nlm.nih.gov/pubmed/29654376
- https://www.ncbi.nlm.nih.gov/pubmed/26512024
- http://care.diabetesjournals.org/content/27/suppl_1/s84
- https://jamanetwork.com/journals/jamaophthalmology/article-abstract/635006?redirect=true
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2761813/
- http://care.diabetesjournals.org/content/33/6/1315
- https://www.ncbi.nlm.nih.gov/pubmed/27889727
- https://www.ncbi.nlm.nih.gov/pubmed/24381884
- https://www.ncbi.nlm.nih.gov/pubmed/22361220
- https://www.ncbi.nlm.nih.gov/pubmed/22244464
- https://www.ncbi.nlm.nih.gov/pubmed/21051047
- http://lillydiabetes.com/_assets/pdf/hi86638_carbohydrate_counting_for_children.pdf
- https://www.mayoclinic.org/diseases-conditions/hyperglycemia/symptoms-causes/syc-20373631
- https://www.mayoclinic.org/diseases-conditions/hypoglycemia/symptoms-causes/syc-20373685
- http://www.lillydiabetes.com/_assets/pdf/ld90766_carbguide.pdf